Emergency War Surgery NATO Handbook: Part I: Types of Wounds and Injuries: Chapter III: Burn Injury
Magnitude of Injury
United States Department of Defense
The severity of thermal injury is dependent upon the depth and extent of the burn. These two factors determine not only mortality and initial treatment requirements, but also morbidity, metabolic consequences of injury, character of healing, and the ultimate functional result.
The extent of the body surface burned can be estimated by employing the "rule of nines." The distribution of surface area by anatomical part in the adult is illustrated in Figure 15, showing the percentage of total skin surface represented by each body part to be: head and neck, 9%; anterior trunk, 18%; posterior trunk, 18%, upper extremities, 9% each; lower extremities, 18% each; and genitalia and perineum, 1%.
To estimate the extent of irregularly disposed burns one can make use of the fact that one surface of the casualty's hand represents approximately 1% of his total body surface. Patients with burns of more than 15% of the body surface typically require some resuscitative treatment and, in most situations, are best cared for in the hospital. Young soldiers tolerate thermal injury best, while older casualties (above 50) and the very young have greater mortality rates for a given extent of burn. The location of the burn influences not only prognosis but also the need for hospitalization. Small burns of the face, hands, feet, or perineum may require hospitalization, even if these limited areas are the only sites of burn injury.
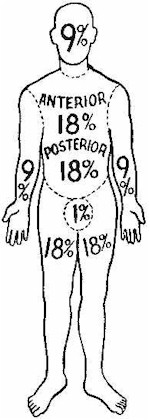
Figure 15