|
The Cervix
The cervix is located at the top of the vagina. It is the
opening to the uterus and is composed of dense connective tissue. It has very
little smooth muscle in it, compared to the rest of the uterus, which is almost
entirely smooth muscle.
The cervix is visualized by placing a speculum in the
vagina. At the top of the vagina is a smooth, pink, firm structure with an
opening (the os) in the center, which leads to the uterus.
|
 The Pap Smear
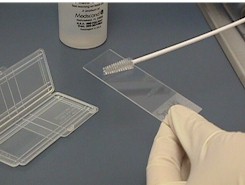
In the 1940's, Dr. Papanicolaou developed a technique for
sampling the cells of the cervix (Pap smear) to screen patients for cancer of
the cervix. This technique has proven to be very effective at not only detecting
cancer, but the pre-cancerous, reversible changes that lead to cancer.
While not originally designed to detect anything other
than cancer, the Pap smear has proven useful in identifying other, unsuspected
problems.
So useful has the Pap smear become, it is considered an
essential part of women's health care. It is typically performed annually in
sexually-active women of childbearing age, although there are some important
exceptions.
Because the Pap smear is a screening test, it can have
both false positive and false negative results. For this reason, it is important
to have the test performed regularly (annually in the military services). It is
not likely that the Pap smear will miss an important lesion time after time.
Pap smears are best performed in a stable, garrison
situation because of the time it takes to send out the smear, have it read, get
the result back, and perform any follow-up care that is needed. The actual
obtaining of a Pap smear can be done almost anywhere (at sea, in the air, in the
field), but getting the results back and further treatment performed in these
operational settings can be difficult or impossible.
Dysplasia
Dysplasia means that the skin of the cervix is growing
faster than it should.
Cervical skin cells are produced at the bottom of the skin
(basal layer). As they reproduce, the daughter cells are pushed up towards the
surface of the skin. As they rise through the skin layer, they mature, becoming
flat and pancake-like (as opposed to round and plump). Their nuclei initially
become larger and darker. If these daughter cells reach the surface of the skin
before they are fully mature, a Pap smear will reveal some immature cells and
"dysplasia" is said to exist.
There are degrees of dysplasia: mild, moderate, and
severe. None of this is cancer, but the next step beyond severe dysplasia is
invasive cancer of the cervix. For this reason, any degree of dysplasia is of
some concern, but the more advanced the dysplasia, the greater the concern.
Mild Dysplasia
Mild dysplasia means the skin cells
of the cervix are reproducing slightly more quickly than normal. The cells are
slightly more plump than they should be and have larger, darker nuclei. This is
not cancer, but does have some pre-malignant potential in some women. Other
phrases that describe mild dysplasia include:
-
LGSIL (Low-grade Squamous
Intraepithelial Lesion)
-
CIN I (Cervical Intraepithelial
Neoplasia, Grade 1)
Many factors contribute the
development of mild dysplasia, but infection with HPV, (Human Papilloma Virus)
is probably the most important. Smoking tobacco products and an impaired immune
system also may contribute to this.
Mild dysplasia can come and go,
being present on a woman's cervix (and Pap smear) at one time and not
another.
Of all women who develop mild
dysplasia of the cervix, about 10% will, if untreated, slowly progress
through the various degrees of dysplasia and ultimately develop invasive
cancer of the cervix. The rest will either remain unchanged or regress back
to normal.
Because so many cases of mild
dysplasia regress, It is common for women who develop a single Pap smear
showing mild dysplasia to be watched over time with the Pap smear being
repeated in 6 months. If the dysplasia persists or worsens, further
evaluation is undertaken. If the Pap returns to normal, the woman's cervix
is followed, sometimes with more frequent Pap smears.
Other physicians feel that the
cervix should be evaluated with colposcopy with even a single dysplastic Pap
smear. Their reasoning is that while many of the Pap smears revert to normal
in 6 months, the abnormality will often re-appear at a later, less
convenient time. They also reason that many women will feel anxiety over
simply observing the abnormality over time and not investigating it right
away. Operational circumstances may well dictate the approach that needs to
be followed.
For women who have previously
been evaluated with colposcopy and found to have dysplasia, the appearance
of mild dysplasia on a subsequent Pap smear is not particularly alarming.
Whether to re-colposcope them and the timing of such a re-evaluation must be
individualized, based on the operational circumstances, the patient's
history, risk factors, the degree of abnormality in the past and intervening
Pap smear results. It is best to consult with an experienced colposcopist or
gynecologist before making a final decision.
Treatment of mild dysplasia may
be cryosurgery (freezing the part of the cervix containing the dysplastic
cells and destroying those cells). Other approaches include vaporizing the
dysplastic cells with a laser, or shaving them off with an electrified wire
(LEEP). Sometimes, the mild dysplasia is not treated at all, but the patient
is closely watched instead. If the dysplasia advances to a more severe
stage, treatment can be undertaken at that later time. But for women in
low-risk situations whose cervical lesion does not advance, surgery can
sometimes be avoided.
Continue
to the PowerPoint Lecture...
|
