|
|
|
Operational Obstetrics & Gynecology
Normal Pregnancy
The diagnosis of pregnancy is accurately made with a urine pregnancy test. Current test kits are highly specific and detect 35-30 mIU of HCG (human chorionic gonadotropin, the pregnancy hormone) per ml of urine. In other words, the pregnancy test will be turning from negative to positive at about the time of the first missed menstrual period.
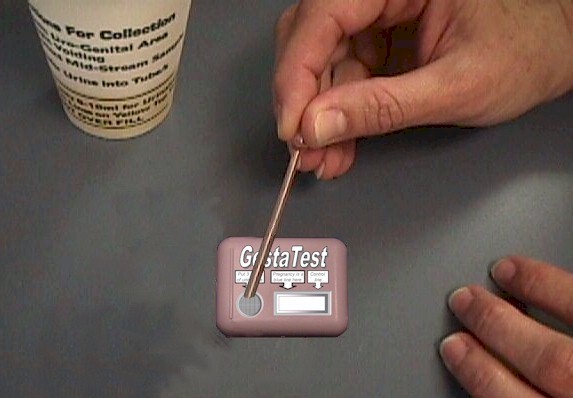
Collect a fresh urine specimen. First morning specimens are preferable in early pregnancy because they are more concentrated and more likely to be positive is only small amounts of pregnancy hormone are present.
Place the correct number of drops of urine in the collecting area of the test kit. The precise number of drops varies from manufacturer to manufacturer.
Wait the length of time specified by the manufacturer.
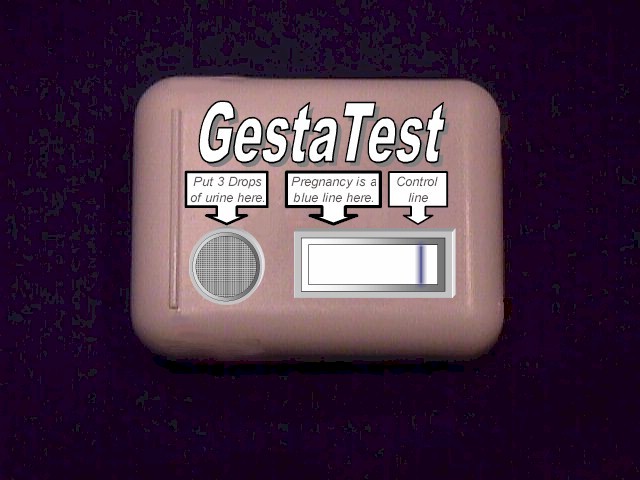
With this particular test kit, the test is read after 3 minutes. A blue line next to "Control Line" indicates that the urine has turned the control area positive. This means the test kit is working correctly.
Because there is no visible "+" in the pregnancy test area, the test results are negative...the patient is not pregnant.
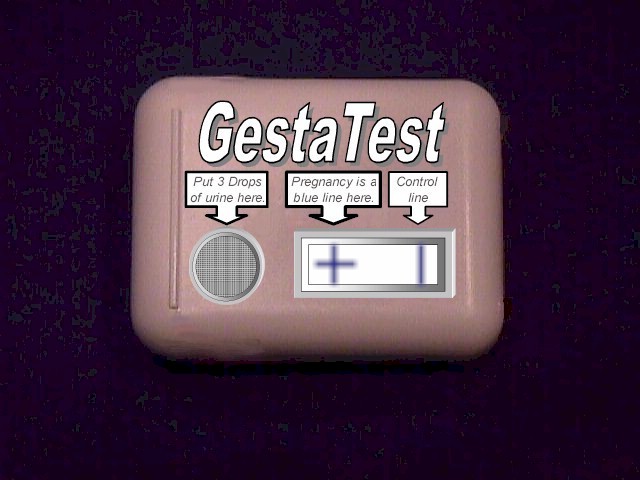
In this case, the control area turned positive, indicating that the test is working correctly.
The test area demonstrates a "+." This means the test is working correctly and the results are positive...the patient is pregnant.
|
|
|
|
In the event of an "equivocal" pregnancy test...one that is not really positive nor negative, additional urine can be put through the test kit to boost the sensitivity. Instead of using 3 drops of urine, you can use up to 6 drops of urine. This will virtually double the sensitivity of the test, while increasing the chance of a false positive by only a small amount.
In an urgent situation, if a patient is unable to provide urine for the test, serum can be used in the urine test kit in place of urine.
- Draw blood into a test tube.
- Tape the test tube to the wall for about 10 minutes (allow it to clot).
- Using an eye dropper or a syringe with a needle, draw off a small amount of serum (the clear, watery part of the blood that's left at the top of the test tube after the blood has clotted).
- Use the serum instead of urine in the urine pregnancy test kit, drop for drop. If the test kit calls for 4 drops of urine, use 4 drops of serum.
This is an imperfect solution, because the forms of HCG (pregnancy hormone) found in serum are somewhat different from the forms found in urine. Further, the serum proteins tend to sludge up the test kit, both mechanically and biochemically. That said, using serum instead of urine will work well enough for most purposes in an operational setting and can provide immediate insight into the patient's problem.
Home À Introduction À Medical Support of Women in Field Environments À The Prisoner of War Experience À Routine Care À Pap Smears À Human Papilloma Virus À Contraception À Birth Control Pills À Vulvar Disease À Vaginal Discharge À Abnormal Bleeding À Menstrual Problems À Abdominal Pain À Urination Problems À Menopause À Breast Problems À Sexual Assault À Normal Pregnancy À Abnormal Pregnancy À Normal Labor and Delivery À Problems During Labor and Delivery À Care of the Newborn
|
Bureau of Medicine
and Surgery |
Operational
Obstetrics & Gynecology - 2nd Edition |
This web version of Operational Obstetrics & Gynecology is provided by The Brookside Associates Medical Education Division. It contains original contents from the official US Navy NAVMEDPUB 6300-2C, but has been reformatted for web access and includes advertising and links that were not present in the original version. This web version has not been approved by the Department of the Navy or the Department of Defense. The presence of any advertising on these pages does not constitute an endorsement of that product or service by either the Department of Defense or the Brookside Associates. The Brookside Associates is a private organization, not affiliated with the United States Department of Defense. All material in this version is unclassified.
This formatting ® 2006
Medical Education Division,
Brookside Associates, Ltd.
All rights reserved